Coronis Health – Anesthesia
Anesthesia Billing
Private-practice, hospital-owned, and university-based anesthesia facilities can rest assured they are in good hands with Coronis Health’s team of anesthesia medical billing and revenue cycle management experts, who use the most innovative technology, like Anesthesia Touch™, to improve revenue.
Our anesthesiology billers provide complete RCM services, from system integration to practice management.
Specialized Solutions, Global Capabilities



Risk-Free Financial Checkup
We Find Missing Revenue In 95% Of Our Reviews
– Comprehensive review of your complete revenue cycle
– Compare key metrics against competitors in your specialty
– Review patient and insurance A/R, charges, and fee schedules
*Rate is based on collections volume
Case Studies
Anesthesia Billing
$872k
increase in revenue

Coronis Health Helped One Hospital Revitalize Its Anesthesia Division with Skyrocketing Revenue
With Coronis’ guidance and leadership, the hospital received a $900K stipend and saw an increase in revenue of $872K (13% in the first year) and 53% in 2014.
$4.5M
increase in revenue

Improving Quality to Attract Top Talent and Increase Revenue
The large medical center’s partnership with Coronis resulted in a complete transformation of their anesthesia services. Coronis’ efforts to address the challenges faced by the anesthesia division resulted in increased stipends, income per shareholder, revenues, and expanded services.
Specializing In Anesthesia Practices
Testimonials
-
35+
Years of Experience
-
7
Specialized Service Groups
-
2000+
Team Members
-
31.2M+
Claims Processed Per Year
-
100%
Transparency
-
$560000
In Charges
-
$180000
In Receipts
Size Matters! More is Always More!
Services

What Makes Us Different
Coronis Health is a global company with a personal, high-touch service. We brought the most innovative and thought-advancing leaders in anesthesia medical billing and revenue cycle management together to progress this industry into the modern, technological age.
-
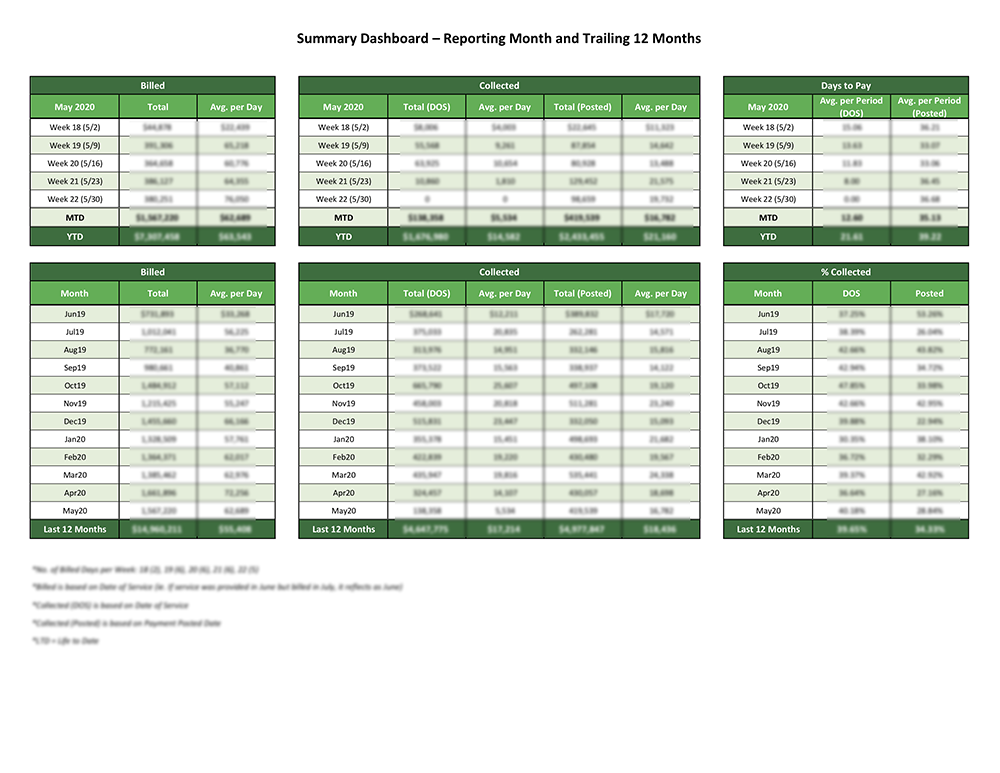
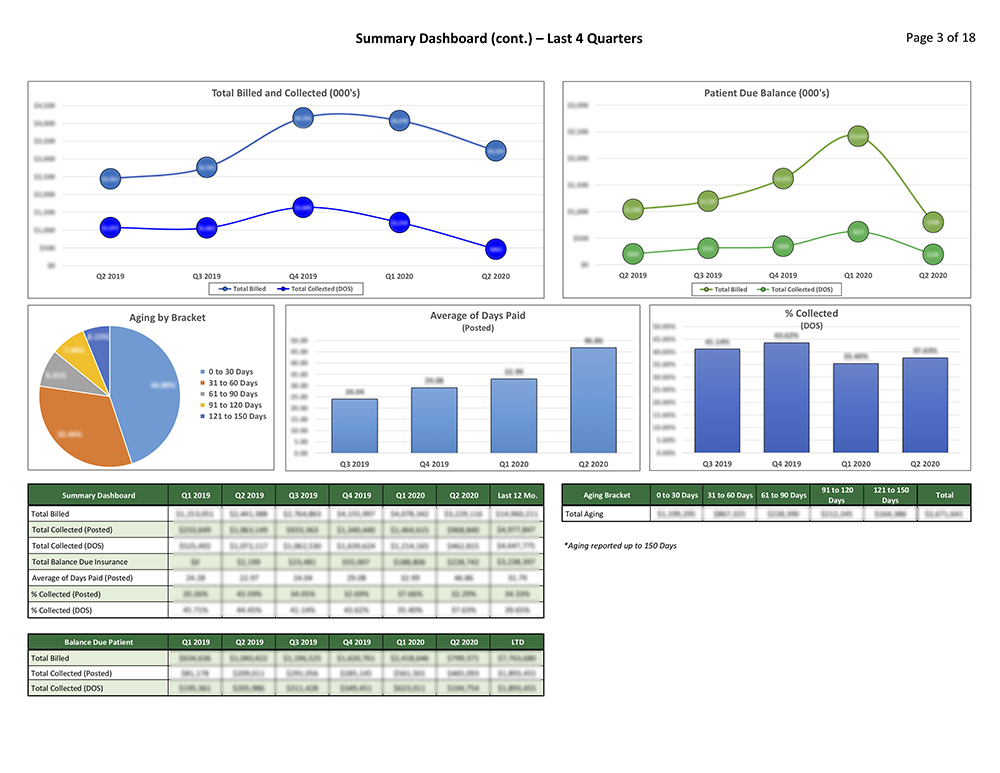
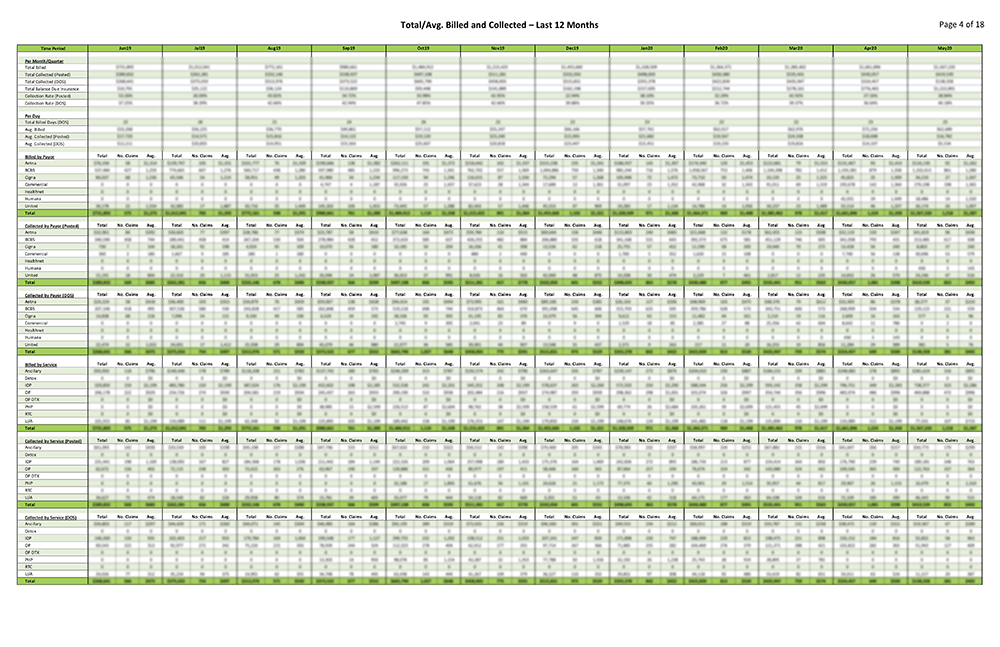
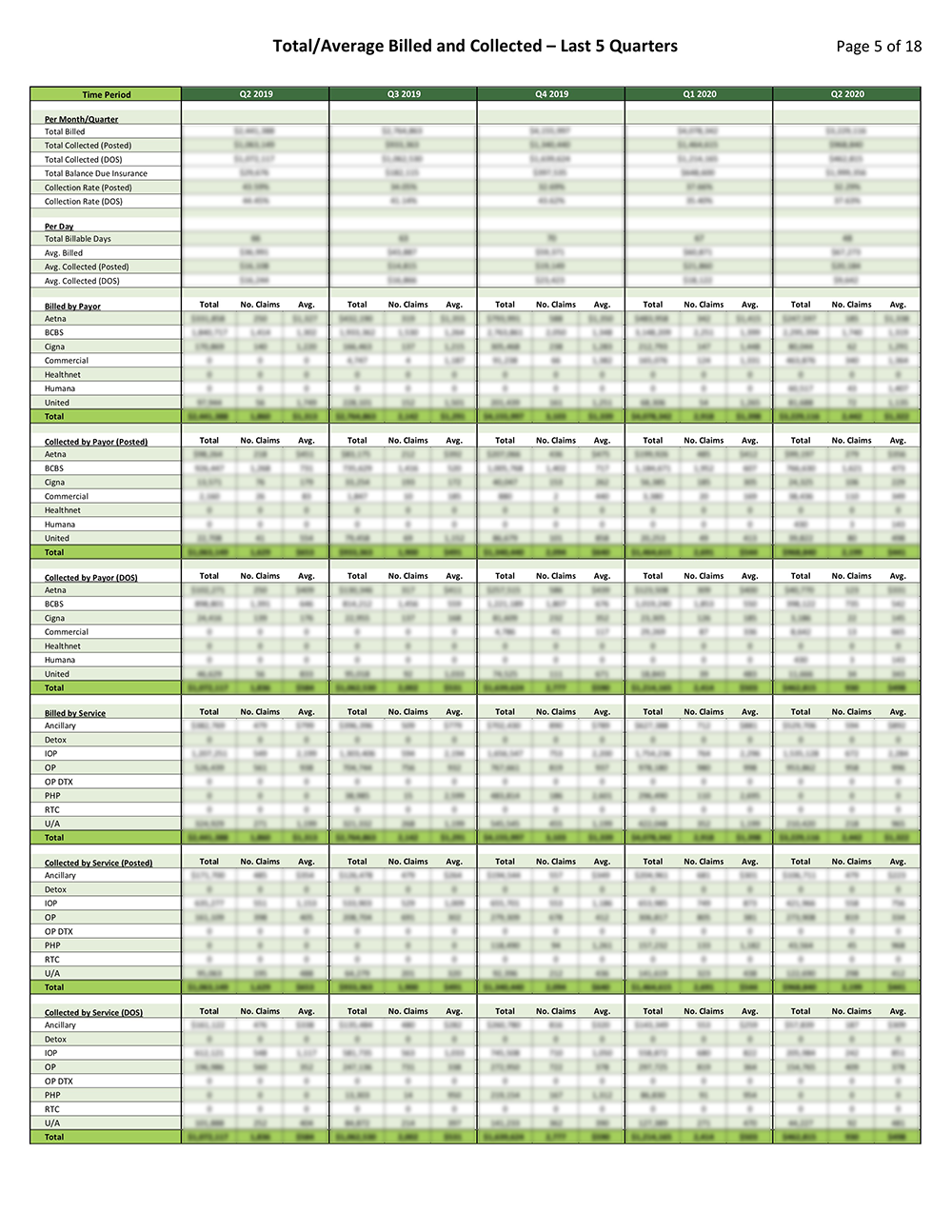
Data-Driven Analysis and Consultation
Numbers only tell half of a story and can often tell that half incorrectly. Our team has experience dealing with complex finances, scheduling, and distribution structures of anesthesia practices, and break down numbers to deliver the real story. When you get a report from us, the WHAT, WHY, and HOW are combined to give actionable intelligence so you can make the best decisions moving forward.
-
Best of the Best in Medical Billing
Coronis Health comprises the top medical billers in the country pooling their global resources to bring customers the best in medical billing and revenue cycle management. With over 100 years of combined experience in various niches including independent and hospital-based anesthesia practices of all sizes, Coronis offers customers tailored solutions and high-touch relationships you won’t find at a “Big Box” medical billing company.
-
EMR/Technology Integration
We are fully integrated with the latest software so we input coding instantly, and execute collections fast and efficiently. And because of our full transparency, you’ll know exactly how your numbers look and how they affect your business.
-
Focused On Your Financial Success
Coronis Health goes after the last dollar using our seasoned team of tireless and tough negotiators. We work hard to get your last 10-15% of missing revenue. You’ll receive timely, relevant, and accurate information in a way you can understand. We don’t help you just get money, we help you financially grow.
-
Personalized Touch
An experienced account manager based here in the United States who understands how to help your practice succeed. You aren’t just a number, you’re on a first-name basis and a phone call away from management. With our transparency guarantee, you see what we see.
More About Coronis Health
Sophisticated anesthesia practices, whether private-practice, hospital-owned, or University-based know that their most important financial asset is their billed services and accounts receivable. This asset needs to be safeguarded, well-organized, tightly managed, and carefully maintained by a professional team possessing a perfectionist approach to execution, accuracy, follow-up, and timeliness. And of critical importance, anesthesia practitioners need to remain constantly vigilant and compliant amid the changing chorus of governmental/carrier billing and documentation regulations and compliance requirements.
